Why Melatonin Does Not Work for Everyone
What Melatonin does
Melatonin is best thought of as a signal for the body to enter its physiological night mode. Research does show that supplementing with melatonin can affect both sleep onset and duration. [1] However, the doses and the way people tend to use it as a supplement are not aligned with how melatonin is typically used in research. Melatonin works best by reinforcing circadian rhythm and shifting sleep timing. It is not a strong sedative that knocks most people out and puts them to sleep.
Here is a list of actions associated with increase of melatonin at night:
Signals “biological night” to the brain
Increases sleepiness and sleep readiness (often helps more with timing than sedation itself)
Lowers core body temperature slightly
Helps shift body towards rest/repair mode
Slower digestion
Lower cortisol and higher growth hormone
Antioxidant signaling
Tissue repair
Decreases blood pressure and heart rate
Adenosine And Sleep Drive
Adenosine is one of the body’s primary sleep pressure signaling molecules. It gradually builds the longer you are awake and creates the feeling of sleepiness. Sleep lowers adenosine. A long late-afternoon nap can reduce adenosine buildup and lower the drive to sleep later that night.
Higher adenosine:
Increases drowsiness
Reduces alertness
Lowers reaction time
Promotes sleep onset
Makes you want to sleep
Caffeine can keep people awake by blocking adenosine receptors.
Cortisol And Stress Response
Cortisol is one of the body’s main stress and alertness hormones. Under normal conditions, cortisol rises in the morning to help promote wakefulness, energy, blood sugar stability, and mental alertness. It then gradually declines throughout the day.
Stress, overwork, illness, inflammation, irregular schedules, or chronic nervous system activation can disrupt this rhythm. In chronic insomnia, cortisol may remain elevated later into the evening. This leads to nighttime alertness, light sleep, or difficulty relaxing despite exhaustion. Patients often describe this as feeling “tired but wired.”
Cortisol itself is not “bad.” It is an important survival hormone. The problem is often not simply high or low cortisol, but disrupted timing and regulation of the overall stress response system.
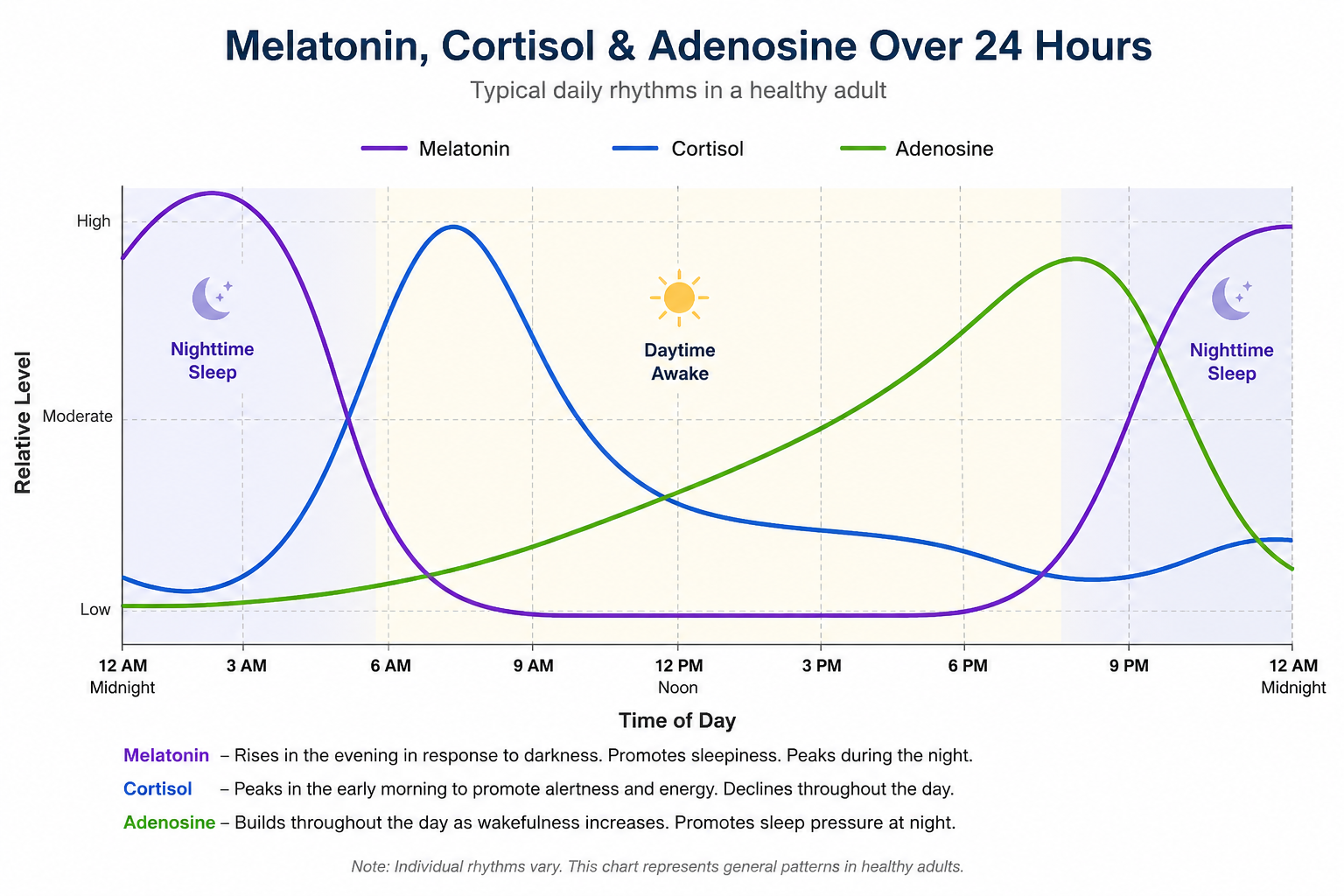
Sleep Hormone Coordination
Melatonin is more like a conductor helping coordinate nighttime physiology than a sedative forcing sleep. It helps tell the body that it is nighttime. It does not guarantee sleep if stress hormones, nervous system activation, inflammation, or disrupted sleep pressure are overriding the signal.
Even adding in adenosine and cortisol this is still an oversimplification. But at least now it should be clear that good sleep requires coordination of:
- Circadian rhythm – Melatonin
- Sleep drive – Adenosine
- Stress response – Cortisol
This is why taking 1 pill of melatonin very often does not work.
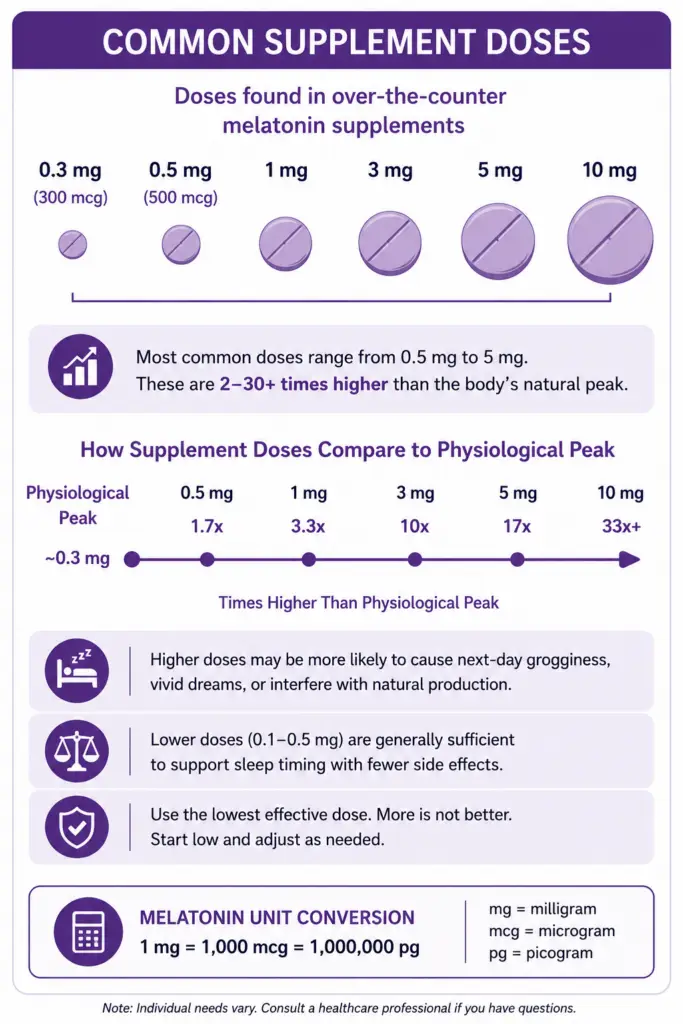
Why Higher Doses Of Melatonin Often Fail
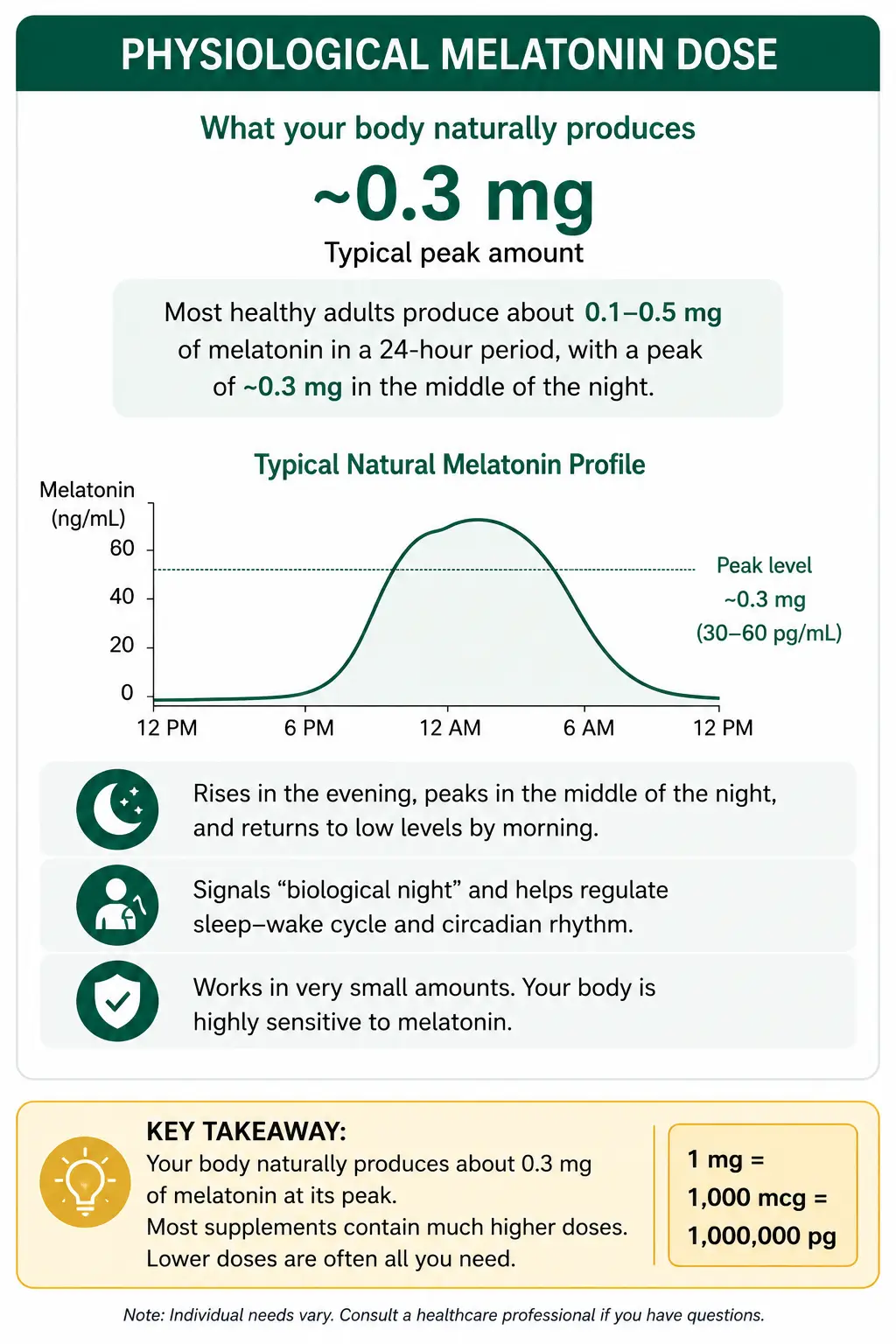
The Physiological dose of melatonin is how much your healthy body would normally make each evening. Most estimates put it at about 0.1mg to 0.5mg.
For a long time many melatonin supplements were sold in 3mg doses. Some companies later began marketing higher-dose melatonin in 10mg and even 20mg. These higher doses were originally explored more for specialized situations than for routine insomnia.
But it didn’t take much time before companies started to market melatonin in 5mg, 10mg or higher for sleep. Research has shown that over the past 20 years, many more people are not just using melatonin. They are taking a higher dose of it. [2]
Higher doses are not always more effective and may sometimes increase grogginess, vivid dreams, or disrupt sleep timing in sensitive individuals.
For difficulty falling asleep, a near physiological dose, taken a few hours before bed time often works best. The larger, typical supplement dose can be much less effective.[3]
Tired But Wired Sleep Patterns
Some people feel tired at night, but when they lay down to sleep, they feel wide awake, or agitated. Their mind can’t stop racing.
A detailed description of this pattern is beyond the scope of this page. But this is often related to the body’s stress response and the hormone cortisol. There are lifestyle adjustments and supplements which can help cortisol. High dose melatonin is typically not one of them.
Another pattern of insomnia is waking up in the middle of the night. This can be related to spikes in cortisol, blood sugar instability, histamine, and sleep apnea. Melatonin may still help support sleep quality in some cases. However, this insomnia pattern is often better addressed with approaches aimed at stress response regulation, blood sugar stability, breathing patterns during sleep, or histamine-related issues.
Circadian Rhythm and Light Exposure
Small circadian rhythm adjustments can sometimes have a surprisingly large effect over time. Helpful foundations may include reducing light exposure at night with blackout curtains, getting bright light exposure in the morning, eating meals at more consistent times, and maintaining a regular sleep schedule. Some people also do better taking Vitamin D earlier in the day and Magnesium later in the evening as part of supporting normal day/night physiology.
These are not “quick fixes,” but rather ways of helping reinforce the body’s natural circadian rhythm. Even small shifts in timing can accumulate over weeks.
How To Use Melatonin
Research from MIT and others suggests that physiological doses of melatonin (around 0.1–0.5 mg) may work differently than the large doses commonly sold in supplements. Additional research also shows that taking melatonin several hours before going to bed, can help shift the circadian rhythm forward. [4] [5] [6]
So, if someone is falling asleep 3:00 AM and wants to move it to 11:00 PM, then they can start taking the low dose melatonin at 10:30 and work on moving their sleep time up from 3:00 AM to 2:30. Once that happens, the dose timing can be moved forward again, until sleep is established at the desired time.
What if taking 3mg of melatonin before bed works for me?
Most of my clients who have told me they’ve tried melatonin say it did not work for them. But there are some people who tell me taking 3mg before bed helps them. Since it’s important to follow individual response, I do not tell these people to change what they are doing.
Treatment Often Goes Beyond Melatonin
Since melatonin is only one part of sleep physiology, treatment often needs to go beyond simply taking a sleep supplement. Improving sleep often requires identifying the specific patterns preventing the body from fully transitioning into nighttime physiology.
Different Sleep Patterns Can Have Different Causes
difficulty falling asleep
waking during the night and not falling back to sleep
light unrefreshing sleep
sleeping but waking exhausted
delayed sleep phase
“tired but wired”
fragmented sleep
Return to the main Sleep and Night Physiology page here
This page is educational and not intended as individualized medical advice.
References
Costello RB, Lentino CV, Boyd CC, et al. The effectiveness of melatonin for promoting healthy sleep: a rapid evidence assessment of the literature. Nutrition Journal. 2014;13:106. doi:10.1186/1475-2891-13-106
Li J, Somers VK, Xu H, Lopez-Jimenez F, Covassin N. Trends in Use of Melatonin Supplements Among US Adults, 1999-2018. JAMA. 2022;327(5):483-485. doi:10.1001/jama.2021.23652
MIT News Office. Scientists pinpoint dosage of melatonin for insomnia. Massachusetts Institute of Technology. October 17, 2001.
Zhdanova IV, Wurtman RJ, Morabito C, et al. Effects of low oral doses of melatonin, given 2–4 hours before habitual bedtime, on sleep in normal young humans. Sleep. 1996;19(5):423–431.
Zhdanova IV, Wurtman RJ, Lynch HJ, et al. Sleep-inducing effects of low doses of melatonin ingested in the evening. Clinical Pharmacology & Therapeutics. 1995;57(5):552–558.
Lewy AJ, Ahmed S, Jackson JM, Sack RL. Melatonin shifts human circadian rhythms according to a phase-response curve. Chronobiology International. 1992;9(5):380–392.